Expert’s Opinion
 Pitavastatin: The Statin with a Difference
Pitavastatin: The Statin with a Difference
Introduction
Pitavastatin is the latest statin to get approval worldwide. It is the competitive inhibitor of 3-hydroxy-3-methyl-glutarylcoenzyme A (HMG-CoA) reductase enzyme. Inhibiting this (rate-limiting) enzyme impedes cholesterol synthesis in the liver, thereby increasing low-density lipoprotein cholesterol (LDL-C) receptor expression which subsequently reduces LDL-C and total cholesterol levels.1 Pitavastatin has many unique properties which makes it different from other available statins. Some of these properties have been described hereafter:
Pitavastatin is more effective in increasing high-density lipoprotein cholesterol (HDL-C) compared to other statins. In an Indian double blind randomised controlled trial, 100 dyslipidaemia patients were randomised to 4 mg/day pitavastatin or 20 mg/day atorvastatin and followed-up for 8 weeks. The increase in HDL-C levels was significantly higher in the pitavastatin group (11%) vs. the atorvastatin group (5.35%) (p<0.001).2 In a sub-analysis of the LIVALO Effectiveness and Safety (LIVES) study in patients with low HDL-C levels who were treated with pitavastatin for 104 weeks, there was a 32% increase in HDL-C levels. Patients who were shifted from other statins to pitavastatin also showed significant increase in HDL-C levels.3
Pitavastatin has significant pleiotropic effects including anti-inflammatory effects which might be beneficial for atherosclerosis regression. In the Kansai Investigation of Statin for Hyperlipidaemic Intervention in Metabolism and Endocrinology (KISHIMEN) trial, dyslipidaemia patients were treated with pitavastatin 1-2 mg for 12 months. Pitavastatin significantly reduced high sensitivity C-reactive protein (hs-CRP) levels by 28.6% in overall subjects and by 62.4% in the highest quartile at 12 months.4
Statin therapy is known to increase blood glucose levels and increase the risk of new onset diabetes in non-diabetic patients.5 Pitavastatin has shown neutral or beneficial effects on blood glucose levels in both diabetic and nondiabetic patients.6 In the Japan Prevention Trial of Diabetes by Pitavastatin in Patients with Impaired Glucose Tolerance (J-PREDICT) study, 1269 patients with impaired glucose tolerance were treated with 1-2 mg pitavastatin or placebo for up to 5 years. There was a significant 18% reduction in the risk of developing new onset of diabetes (Figure 1).7
Pitavastatin has been shown in many studies to be well tolerated in patients who are intolerant to other statins. In a study, 3 out of 4 (76%) patients who were intolerant to >2 statins were able to tolerate pitavastatin for 6 months.8 Better tolerability of pitavastatin is possibly due to a lower decrease in coenzyme Q10 (CoQ10) compared to other statins.9 Pitavastatin should be considered a preferred statin when a patient requires statin therapy but fails to tolerate other statins.
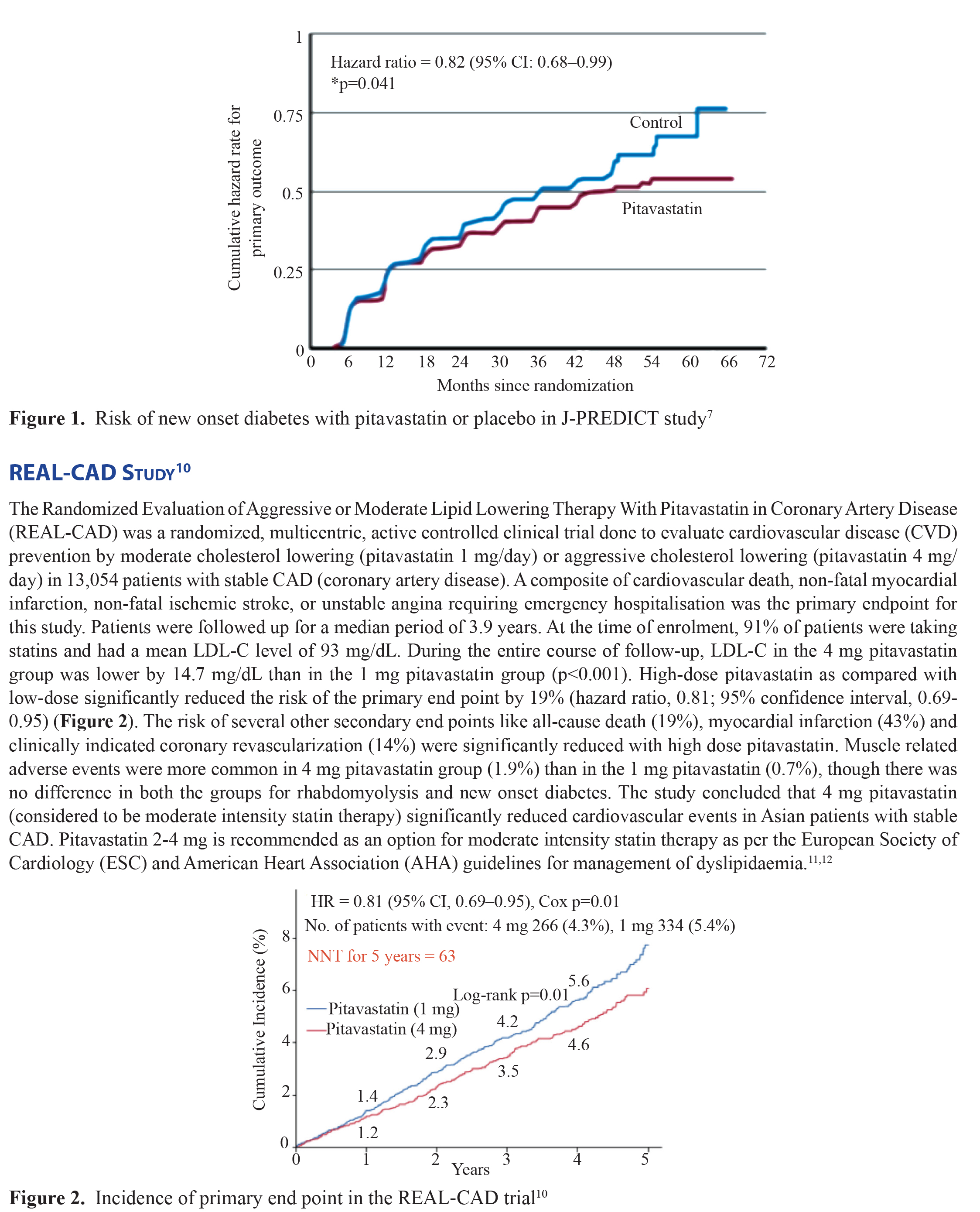
The REAL CAD is the first cardiovascular outcome study comparing different intensities of statin therapy in Asianpatients for secondary prevention. Success of this trial has opened newer horizons for management of dyslipidaemia by socalled “moderate” intensity statin (4 mg pitavastatin) in Asian patients suffering from CAD.With several studies documenting unique benefits with the use of pitavastatin, it undoubtedly is the statin with a difference.
Summary
Pitavastatin is an extensively studied molecule. It elevates high-density lipoprotein cholesterol (HDL-C), has anti-inflammatoryeffects and salutary effect on blood glucose. It is the best tolerated drug of its class and is one of the few members of its classto have data documenting secondary prevention of cardiovascular disease.
Declaration of conflicting interests
The authors declare no conflict of interest.
Funding
No funds were received for publishing this article.
References
1. Hoy SM. Pitavastatin: A Review in Hypercholesterolemia. Am J Cardiovasc Drugs. 2017; 17(2):157-168.
2. Patil CY, Baig MS, Doifode SM. Assessing the efficacy and safety of pitavastatin compared to atorvastatin in dyslipidemicpatients: a double blind randomized controlled trial. Int J Basic Clin Pharmacol. 2016; 5:834-40.
3. Teramoto T. The clinical impact of pitavastatin: comparative studies with other statins on LDL-C and HDL-C. Expert OpinPharmacother. 2012; 13(6):859-865.
4. Fujioka Y, Fukuda A, Ishida T, Kagimoto S, Nakamura Y, Iwakura A, et al. Pitavastatin reduces elevated IL-18 levels inJapanese subjects with hypercholesterolemia: sub-analysis of Kansai investigation of statin for hyperlipidemic intervention inmetabolism and endocrinology (KISHIMEN). J Atheroscler Thromb. 2011; 18(1):8-15.
5. Sattar N, Preiss D, Murray HM, Welsh P, Buckley BM, de Craen AJ, et al. Statins and risk of incident diabetes: a collaborativemeta-analysis of randomised statin trials. Lancet. 2010; 375:735-42.
6. Teramoto T, Shimano H, Yokote K, Urashima M. New evidence on pitavastatin: efficacy and safety in clinical studies. ExpertOpin Pharmacother. 2010; 11(5):817-28.
7. Arnaboldi L, Corsini A. Could changes in adiponectin drive the effect of statins on the risk of new-onset diabetes? The case ofpitavastatin. Atheroscler Suppl. 2015; 16:1-27.
8. Friedrich DA, Ziajka PE, Smith JO. Pitavastatin Use in Patients with Previous Statin Intolerance. J Clin Lipidol. 2012; 6(3):274.
9. Kawashiri MA, Nohara A, Tada H, Mori M, Tsuchida M, Katsuda S, et al. Comparison of effects of pitavastatin and atorvastatinon plasma coenzyme Q10 in heterozygous familial hypercholesterolemia: results from a crossover study. Clin Pharmacol Ther.2008; 83(5):731-39.
10. Taguchi I, Iimuro S, Iwata H, Takashima H, Abe M, Amiya E, et al. High-Dose Versus Low-Dose Pitavastatin in JapanesePatients With Stable Coronary Artery Disease (REAL-CAD): A Randomized Superiority Trial. Circulation. 2018; 137(19):1997-2009.
11. Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Managementof Dyslipidaemias. Eur Heart J. 2016; 37(39):2999-3058.
12. Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on thetreatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College ofCardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014; 63:2889-934.